Vaccine Schedule for 0-6 yr olds.
Click here.
Vaccine Schedule for 7-18 yr olds.
Click here.
Dr. Knapp's personal choices in these vaccine recommendations.
I have adapted the above schedule to help not giving so many shots at one time.
Many are now required for starting Kg and 7th grade in Texas. The
shots below are required.
| Birth |
|
|
|
|
not if
Mom neg test |
|
|
|
| 2months |
Pentacel
#1 |
|
|
PCV#1 |
|
|
|
Rotavirus |
| 4months |
Pentacel #2 |
|
|
PCV#2 |
|
|
|
Rotavirus |
| 6months |
Pentacel #3 |
|
|
PCV#3 |
HepB#1 |
|
|
Rotavirus |
| 9months |
|
|
|
|
HepB#2 |
|
|
|
| 12months |
|
HIB |
HepA |
PCV#4 |
|
MMR#1 |
|
|
| 18months |
DaPT#4 |
|
HepA |
|
HepB#3 |
|
Varicella
1 |
|
| 4yr |
DaPT #5 |
IPV#4 |
|
|
|
MMR#2 |
Varicella 2 |
|
| 12yr |
Tdap |
Menatra |
|
HPV
(3 shots over 6 months) |
|
or
Varicella 2 here |
|
| 17-18yr |
|
Menatra |
|
|
|
|
|
A combination of vaccines were released called the Pentacel that contains DaPT, IPV, and HIB all in one shot. So that
will mean fewer needles especially at 2,4,and 6 months. At 2 months
the baby gets two shots: Pentacel and Prevnar(PCV).
IF there is a shortage we give four shots: DaPT, IPV, HIP, and Prevnar.
I am now recommending not give the HepB vaccine at birth unless the mother
is Positive for the virus. Studies show that the immunity is better in
the teenage years if the vaccine is given at 6 months or later. The
infant is not exposed to the virus except at birth or as an adult. Also as
mothers are coming to us having been vaccinated to HepB, then we need to
wait until their antibodies (that goes through the placenta to the baby)
decrease and not affect the infants vaccination.
Texas is requiring the Tdap, Menatra and a second Varicella (chicken pox) before 7th grade as of Fall 2009. At 12 yr
we give a new Tetanus booster with Pertussis
(Whooping Cough) called a Tdap. This has to be 5 yrs or more past the last tetanus
shot so if you had one at 12-14 yr, then you cannot have one for 5 yr after
that. Also a vaccine called Menatra. This is for Meningiococcal
Meningitis. It is required by most colleges, we have given it for
many years to 12 yr olds, and now required by Texas to enter the 7th grade.
The second Varicella vaccine is required
unless the parent signs a form at school that the child had the chicken pox
illness.
I recommend the Human Papilloma Virus Vaccine (HPV) by 12-13 yr. old
girls and boys.
The virus causes cervical cancer, cancer of the mouth, genital warts,
rectal cancer, nodules on the vocal cords, and prostate cancer. The virus
DNA is found in more than 50% of prostate cancer and none in normal
prostates. It is 3 shots over 6 months: one initially, one 2 months
later, and the third 4 months after the second one.
This vaccine does not increase the promiscuity rate. It is safe and I
strongly recommend it. 10% of the population have the virus by 20 yr old,
50% by 26 yr old, and 80% by 50 yr old. Plus you could be a virgin at
30 yr and marry a spouse with the virus. The virus ends up in both the
groin and mouth so there are people who contract this virus through kissing!
Lately the recommendation is to test for the HPV before or instead of doing
the pap smear! It is that coorelated!
http://triblive.com/news/healthnews/5761200-74/hpv-test-pap#axzz2w52EFL00
HepA is now required for Kg. It is recommended for high risk groups
in the teens who have not had it. Especially they need it if they go
to under developed countries with poor sanitation. Or if they go into
health care fields like paramedics, doctors, nurses, etc.
The Rotavirus vaccine is a vaccine against a "stomach" virus with
vomiting and diarrhea. It is not required for school. It
decreases illnesses and hospitalizations. .
AND NO ...... THE VACCINES DO NOT CAUSE AUTISM!!!
For those parents who have been brainwashed by Dr. Sears.
Please read this article:
Dr Robert Sears, The Vaccine Book: Making the Right
Decision for Your Child.
http://www.forbes.com/sites/emilywillingham/2014/03/23/worried-about-measles-dont-call-dr-bob-sears/
Dr. Knapp
Also see:
http://www.huffingtonpost.com/jennifer-raff/dear-parents-you-are-being-lied-to-about-vaccines_b_5112620.html
Less autism with vaccine:
http://www.psmag.com/health-and-behavior/another-case-for-vaccination
Vaccine schedule from CDC:
http://www.cdc.gov/vaccines/recs/schedules/child-schedule.htm
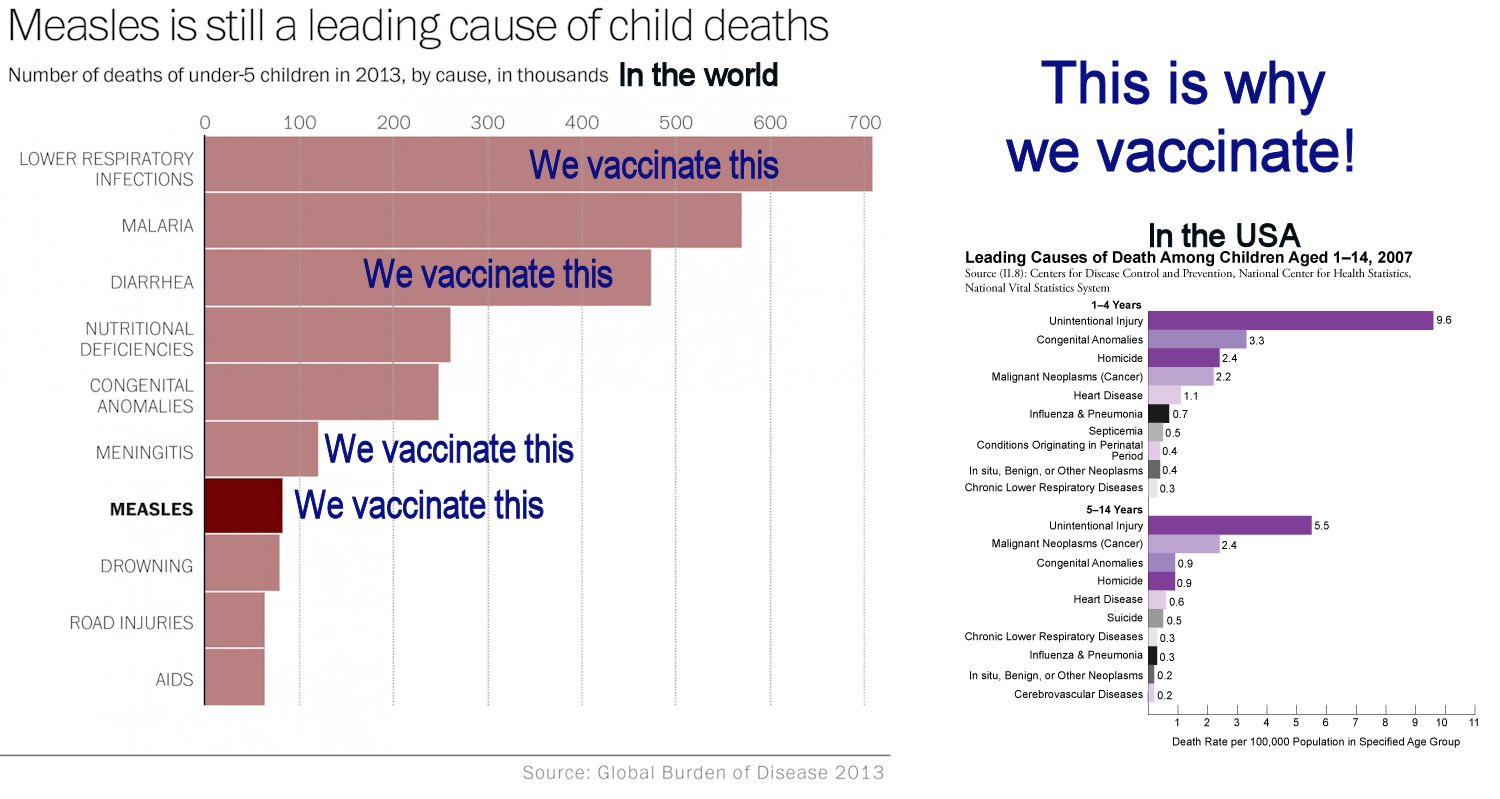
Why Vaccinate?
Web sites with more info:
1.
www.cdc.gov
2.
www.vaccinealliance.com
3.
www.vaccine.org
4.
www.immunize.org
5.
www.immunizationinfo.org
6.
www.fda.gov/oc/opacom/kids/html/vaccines.htm
7. www.who.int/vaccines/
Here are research papers proving there is no connection with
autism and vaccines or thymersol (mercury).
http://sdsma.org/pdfs/09%20-%20History%20of%20Autism%20-%20Blake.pdf
http://lifevesselbeverlyhills.com/val/Vaccine%20Autism.pdf
http://www.sciencedirect.com/science/article/pii/S0264410X12005828
http://journals.lww.com/pidj/Abstract/2010/05000/Lack_of_Association_Between_Measles_Mumps_Rubella.3.aspx
http://pediatrics.aappublications.org/content/126/4/656.short
http://www.tandfonline.com/doi/abs/10.1080/10810731003780714
http://www.landesbioscience.com/journals/vaccines/article/12217/News-PolicyHV6-5.pdf?nocache=179268593
http://www.theannals.com/content/45/10/1302.short
Here are news reports that are interesting:
http://www.mamamia.com.au/social/vaccination-growing-up-unvaccinated/
mother's experience when she herself was not vaccinated.
http://www.geo.tv/GeoDetail.aspx?ID=102691
http://www.nydailynews.com/new-york/brooklyn/measles-outbreak-hits-jewish-neighborhoods-brooklyn-article-1.1346446
http://www.redorbit.com/news/health/1112852881/measles-outbreak-england-call-for-action-concerns-autism-052113/
http://pediatrics.about.com/b/2013/05/28/measles-is-back-and-so-are-the-consequences.htm
http://www.dailytelegraph.com.au/news/opinion/crackpot-crusaders-putting-our-kids-at-risk/story-fni0cwl5-1226641441502
Dr. Knapp
Here
are only a few tombstones in a cemetery from 120+ years ago. This is
why we vaccinate!